Serious games can provide opportunities for high-frequency practice using “low-dose” simulation congruent with the principles of deliberate practice and enable us to measure individual competence in a highly granular way while enabling cognitive skills development anytime, anywhere. Today’s article was guest authored by James Kimo Takayesu MD MS FACEP, Co-Founder of Minerva Medical Simulation, who takes a look at Serious Games in Medical Simulation and education. Following, we share more about FULL CODE, a serious game “app” for ER Simulated training!
When you think about a video game, you might imagine it primarily as a form of entertainment – something for enjoyment and diversion. However, in addition to being entertaining, video games can be incredibly challenging and frustrating, requiring iterative practice in order to achieve various tasks after multiple failures. From Galaga to Myst, Halo to Clash of Clans, video games have the capacity to make people practice until perfect. Modern video games have become increasingly complex, involving a wide array of performance levels of gameplay and multiple players simultaneously in a common virtual environment, all engaged in learning how to achieve. Why do we keep trying in the face of failure? What motivates us to continue playing until we achieve mastery?
Video games have tremendous educational potential. They provide a private learning experience that is judgment-free – a “psychological moratorium of practice” as described by psychologist K. A. Ericsson. They provide opportunities for high-frequency deliberate practice and iterative skill development. As such, serious video games can add a significant learning value to almost any educational curriculum. Serious games can augment an educational experience by engaging learners in active cognitive experiences, providing opportunities for knowledge application and decision-making (Gee, 2003) helping learners to consolidate and assimilate new knowledge much the same way as outlined by educational theories of Bruner, Piaget, and Whitehead. There is clear evidence of their potential. Serious games such as Gran Turismo (driving/auto racing simulation) and Zwift (cycling simulation) create virtual environments for serious gameplay that have developed individuals who have gone on to become professionals, demonstrating the power of serious gaming when the game design is aligned with real world performance.
The apprenticeship model of clinical learning – more familiarly called “see one, do one, teach one” – has traditionally formed the foundation of learning and competency development in the medical field. This requires a breadth of real world experience in order to accumulate the essential skills and knowledge to practice independently. Apprenticeship learning is dependent upon exposure – the chance of encountering a specific disease state over a fixed training time. Knowing that the breadth of clinical exposure is a function of both time and serendipity means that a great deal of hours and effort can be spent performing repetitive cognitive skills, waiting for a new learning experience to expand knowledge and skills. Across a cohort of learners, apprenticeship learning leads to inconsistent exposure over a fixed training time, resulting in heterogeneity of knowledge and clinical skills.
Manikin-based simulation creates these learning experiences in a risk-free environment. One can directly observe individuals learn, practice, and demonstrate their competence managing various disease states and rare high-risk cases. With the addition of a simulation curriculum, one can compress experiences that may take years to come across in the clinical environment to supplement experiences in the clinical learning environment. Engaging clinicians in applied conceptual learning exercises is a cornerstone to effective learning (Armstrong & Parsa-Parsi, 2005). Following the Kolb Learning Cycle, teaching with simulation can provide invaluable opportunities for active experimentation with new concepts that can be reinforced in the clinical environment through concrete experience. Simulation is an accelerant on the fire of learning.
Simulation-based assessments can provide opportunities to directly observe and assess individual learner performance in specific core competencies as well as milestones in learning with a high degree of specificity and accuracy. However, reliance upon the clinical learning environment and focused simulation-based activities is still limited in several important ways. While manikin-based simulation is highly valuable, it can be very costly in terms of the physical resources needed to create a simulation room or lab as well as the significant time constraints of both teaching faculty and learners to be physically present in the simulation lab for a learning or assessment session. These issues limit the frequency of opportunities for regular focused cognitive practice and the number of observations of individual learners that can be made over the course of training. They also limit our ability to determine competency across a wide array of disease states, rare conditions, and clinical management scenarios.
Direct observation of an individual performing a history and physical examination by a trained faculty member using standardized checklist does not deal with the “sampling issue” – infrequent opportunities to measure an individual’s performance lead to an incomplete picture of their competence in the clinical learning environment (Miller 1990). While manikin-based simulation can increase these opportunities, they can be augmented even further using a serious gaming simulation environment (SGSE).
A serious game can provide opportunities for high-frequency practice using “low-dose” simulations, compressing a 30-minute manikin simulation into a 3-minute simulation game that requires the same cognitive skills and applied knowledge. Unlike most manikin-based simulations, SGSE can provide opportunities for repetitive practice and iterative skill development, covering a broad array of diseases, freed from the constraints of physical space and scheduled time. SGSE can motivate performance despite failure because of the privacy of the gaming learning environment, allowing for more challenging cases and complex learning with a low cost of failure and high reward for success. The psychological moratorium that SGSE can provide promotes practice despite failure, as a video game does, to enable practice until successful performance. This can be leveraged to augment performance and prepare learners prior to entering the more high-cost, high-stakes manikin-based simulation environment where the fear of public failure and judgment might impede learning. When used prior to a classroom or simulation training session, a serious video game can calibrate a group of individuals to a common level of performance and understanding prior to engaging in a team simulation exercise.
Ericsson’s concept of deliberate practice relies on four components: a task with a well-defined goal, motivation to improve, feedback on how to improve performance, and the opportunity for repetition, refinement and skill development (Ericsson, 2008). A serious game can enable repetitive practice. Situating serious games within the hierarchy of clinical learning, one can envision didactic learning being the foundation of knowledge acquisition, followed by gaming for initial application of knowledge and skills practice. This preparation can then support higher-level manikin-based simulations which, along with repetitive concept reinforcement with gaming, support real world performance in the clinical learning environment.
Deliberate practice is not just for improving performance – it provides evidence of competence. Tracking individual performance improvement over time with a serious game allows the collection of hundreds, if not thousands, of observations over a relatively short period of time, well within the scope of health professions training. These data can provide evidence of skill acquisition from novice to expert (Dreyfus & Dreyfus, 1980). For example, using a set of 50 simulation cases that can be played repetitively as a serious game, each with specific measurable elements of history, physical, diagnostic testing, and clinical interventions, one can measure thousands of critical actions successfully performed over time through iterative practice to more accurately assess achievement of milestones in training.
In addition to observations from the clinical learning environment and mannequin-based simulations, SGSE can provide a broad and accurate representation of an individual’s clinical competence across a wide array of disease states, from the common to the rare, benign to the critically ill. Put simply, a serious game enables us to measure individual competence at a highly granular way using the principles of deliberate practice while enabling cognitive skills development anytime, anywhere.
About Full Code Emergency Room Simulator
Minerva Medical Simulation is dedicated to the mission of bringing medical simulation to the widest possible audience; to improving quality in medical training and thus overall quality in patient care. Their game, FULL CODE, is the world’s first smartphone-based patient simulation for institutions. Their concept of “high-frequency, low-dose” training focuses purely on decision-making with over a hundred actions to choose from. Each case has a peer-reviewed scoring rubric and debrief to provide granular competancy-based feedback. Their diverse case library allows providers to individualize learning and refresh knowledge in specific areas.
FULL CODE delivers the innovative cognitive training your education team is looking for at a fraction of the cost of existing simulation tools. If you already use manikin-based simulation, FULL CODE is designed to help your learners save time and improve their learning prior to entering the sim lab. “Baseline” your learners by assigning cases before manikin-based simulations to ensure everyone has a practical understanding of core concepts, and then focus on teamwork, communication and systems-based practice. FULL CODE provides for:
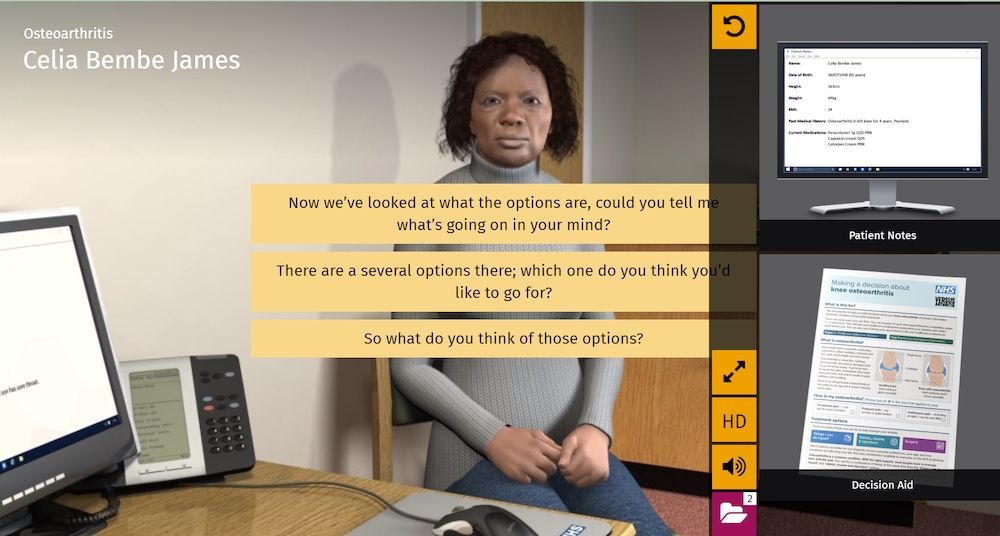
- Realistic Patients: Each has a unique history, realistic vitals, accurate lab results and imagery. Ask the patient questions to start the case.
- Investigate & Diagnose: Examine the patient and formulate a differential diagnosis. Then perform bedside tests, order labs and imaging scans.
- Treat & Hand-off: Choose from among dozens of possible medications, procedures, and consults to treat the patient. Then choose your final diagnosis and hand-off the patient.
- Scoring & Debrief :Every case has a unique scoring rubric and every action you perform affects your final score. The case ends with a detailed written debrief.
- Detailed & Open-ended: No multiple-choice questions here! Choose from 100+ actions, 100+ diagnoses and reveal dozens of patient-specific clinical results & images.
- Realistic 3D Scene: Look in any direction, tap on equipment to perform actions, and the scene evolves as you interact with the patient.
Check out the FULL CODE ER Serious Game Here!
References:
- Armstrong E, Parsa-Parsi R.How Can Physicians’ Learning Styles Drive Educational Planning? Acad Med. 2005; 80:680–684.
- Dreyfus SE, Dreyfus HL. A five-state model of the mental activities involved in directed skill acquisition. University of California, Berkeley, CA: Operation Research Center Report 80-2, 1980.
- Ericsson KA. Deliberate practice and acquisition of expert performance: A general overview. Acad Emerg Med, 2008;15:988-994.
- Gee, JP. What Video Games Have to Teach Us About Learning and Literacy. Palgrave-MacMillan: New York, NY, 2003.
- The ACGME Emergency Medicine Milestones in Training; https://www.abem.org/public/publications/emergency-medicine-milestones, accessed January 3, 2019.
- Miller GE. The Assessment of Clinical Skills/Competence/Performance. Acad Med. 1990;65(9):S63-67.
Have a story to share with the global healthcare simulation community? Submit your simulation news and resources here!